|
Streptococcus pyogenes infection Streptococcal pharyngitis is caused by streptococcus pyogenes. Streptococcal pyogenes is associated with pharyngitis in children. Pharyngitis is best detected via rapid strep test. Streptococcus pyogenes may be transmitted via direct contact or respiratory droplets. Streptococcus pyogenes is a gram positive coccus which is sensitive to bacitracin. Streptococcus pyogenes is lancefield group A with beta hemolytic properties. The virulence factors of streptococcus pyogenes may include structural component such as M protein,( M protein autoantibodies may lead to rheumatic fever due to it cross react with the heart muscle) M - like protein, F protein and hyaluronic acid capsule, enzymes such as hyaluronidase, DNase, C5a peptidase, streptokinase, streptolysin O and streptolysin S as well as erythrogenic superantigen toxins such as Spe A, Spe B and Spe C. Anti streptolysin O antibodies ( ASO) is useful in detecting any streptococcus pyogenes infection in cases of patient with rheumatic fever. Besides pharyngitis, streptococcus pyogenes may also present with Scarlet fever. Scarlet fever is characterized by diffuse rash, strawberry tongue and fever. Other infections may include skin infections due to breaks and cut of the skin. These include, erysipelas, impetigo, necrotizing fasciitis. Other conditions may include streptococcal shock syndrome, sepsis, acute glomerulonephritis and rheumatic fever. The treatment may include surgical debridement in cases of skin lesions or penicillin as well as erythromycin.
0 Comments
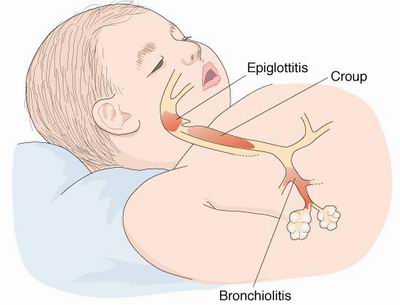
Croup Croup is also known as laryngotracheobronchitis. Croup may present with symptoms and signs such as barking cough, fever, hoarseness and inspiratory stridor. The common causes of croup may include parainfluenza virus type 1 and parainfluenza type 2. There are four types of parainfluenza virus serotypes. Parainfluenza virus type 1, 2, 3 and 4. Types 1 and 2 causes croup. Types 3 parainfluenza virus effect the children and presented with pneumonia and bronchiolitis. Type 4 parainfluenza virus is associated with mild case of upper respiratory illness. The common mode of transmission is respiratory droplets. Parainfluenza virus may infects and damage the respiratory epithelial cells. There will be multinucleated giant cells. Parainfluenza virus is detected by detecting the present of parainfluenza virus specific antibodies and due to culture study. Nasal aspirates may be useful in detecting the present of viral antigens. The common virulence factor for parainfluenza virus may include viral fusion protein.
 Hepatitis E Hepatitis E may present with symptoms and signs of viral hepatitis such as jaundice, fatigue, anorexia, malaise, nausea, vomiting, and upper right upper quadrant pain ( hepatic pain). The most common cause of acute hepatitis is hepatitis E and hepatitis E is not associated with chronic infection. Hepatitis E is caused by hepatitis E virus which is a calicivirus. Hepatitis E virus is detected by Hepatitis E virus specific IgG or IgM antibody. There is no carrier state in hepatitis E infection. The common mode of transmission may include fecal oral route. Hepatitis E occurs due to poor sanitation. The common complication of hepatitis E may include fulminant hepatitis which occur in pregnant women during their third trimester.  Genital Warts Genital warts is also known as condyloma acuminata. Genital wart is caused by human papillomavirus. The common mode of diagnosis is through the pap smear test which evaluate the cytological structure of the cervix. Pap smear also remains the gold standard for detecting cervical cancer. Other modes of investigations may include polymerase chain reaction and hybridization of the DNA. The modes of transmission is via sexual route. There are different types of human papilloma virus. Human papilloma virus types 1, 2 and 4 is related to common warts which present on the feet and on the hands. Human papilloma virus 6 and 11 may cause benign external genital warts and may lead to laryngeal papillomas in children infected in birth canal from mother who suffer from genital warts. Human papilloma virus 16 and 18 are associated with cervical cancer and head as well as neck cancer. Human papilloma virus infection may resolve, remain latent or progressing later into dysplasia / carcinoma. Genital wart or condyloma acuminata can be diagnosed clinically. Human papilloma virus may gain entry to the basal epithelial cells from the cracks, lacerations or tears of the mucosal surface or skin via sexual intercourse. The common treatment may include cryotherapy or laser therapy in removing the genital warts or application of chemical agents such as trichloroacetic acid or podophyllin to remove the wart. Other alternative may include imiquimod.
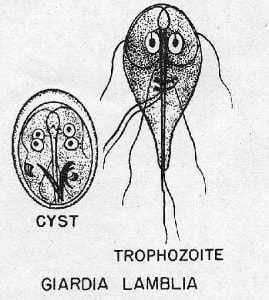
Giardia lamblia infection Giardia lamblia infection may present with watery diarrhea to malabsorption syndrome. Patient with malabsorption syndrome may complain of abdominal cramps and other signs and symptoms such as steatorrhea / fat in the stool, flatulence and foul smelling stools. Patient may be symptomatic and asymptomatic. Patient will shed the cysts in the stools.The cysts will lead to trophozoites which appear in the stools as pear shaped with ventral sucking disk and four flagella. The common mode of transmission may include fecal oral route, oral - anal route and ingestion of cyst from the contaminated water with feces. The common source of infection may include fecal contamination of the mountain stream by muskrats or beavers. Giardia lamblia is an intestinal flagellate which via ventral sucking disk of the trophozites may attach to the duodenum and jejunum. This will block the absorption of fat. The treatment may include proper hygiene and avoiding water from mountain stream. The medication require may include quinacrine hydrochloride and metronidazole.
Tuberculosis Tuberculosis is caused by mycobacterium tuberculosis which is an acid fast rod. The direct examination of the sputum may reveal the present of acid fast bacilli. The reactivity to the purified protein derivative or PPD skin test is also considered. to identify the cell mediated immune response to the cell wall protein component. Mycobacterium tuberculosis is a slow growing bacteria with mycolic acid in the cell wall. Mycobacterium tuberculosis may replicate in the macrophages which resulted in the formation of tubercle ( granuloma) with caseous necrotic center. Granuloma may present in other organs due to erosion of the tubercule which spread to other organs via bloodstream. The caseous necrotic centers may undergo liquefaction and cavitation which progress into active disease. The reactivation of mycobacterium tuberculosis occur due to survival of the organism in the tubercles mostly in immunosuppression patient. The common mode of transmission may include respiratory droplets. Patient may present with active pulmonary disease such as hemoptysis, fever, cough, loss of weight and sweat at night. Mycobacterium tuberculosis may be associated with chronic meningitis. The treatment may include isoniazid, ethambutol, rifampin and pyrazinamide. The treatment is based on the susceptibility testing. Culture with special media is considered while testing for drug resistance. Vaccination with live mycobacterium form related species such as bacillus Calmette Guerin or BCG or chemoprophylaxis is considered.
Amebic Dysentery Amebic dysentery may present with symptoms such as tenesmus, abdominal cramps, stool containing mucus and stool containing blood as well as flatulence. The severe cases of amebic dysentery may present with hepatic abscess. Amebic dysentery may be caused by entamoeba histolytica a form of ameba. There are two forms of ameba which include cyst and trophozoite. The cyst is metabolically inactive and resistant to any change in the environment.The cyst is the active form of ameba which is upon ingestion may lead to excystation and result in formation of trophozoite. Trophozoite ( the active form of ameba) will continue to divide and finally infect the large intestine. This will finally lead to flask shaped ulceration due to destruction of the tissue. The common mode of transmission may include oral anal or fecal oral routes. The infected individual may shed the cyst in the stool. The stool may contaminate the water and food. Entamoeba histolytica can be detected by microscopic examination of the stool which may reveal the present four nuclei cyst and ingested erythrocytes. Patient is advised for proper sanitation and personal hygiene. The treatment for amebic dysentery may include metronidazole, iodoquinol and diloxanide furoate. 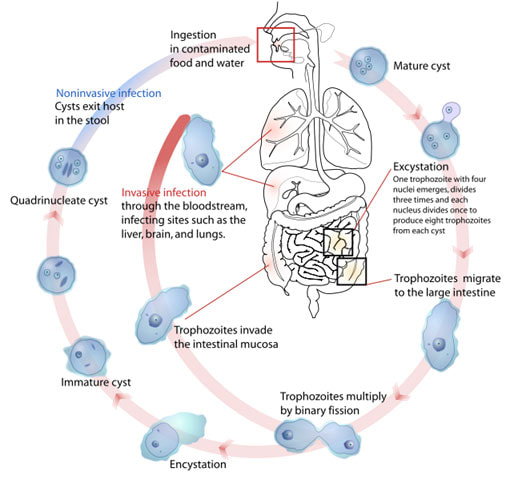 Atypical Pneumonia Atypical pneumonia may be caused by mycoplasma pneumoniae. Serological testing may detect the present of mycoplasma penumoniae. Mycoplasma pneumoniae consists of sterols containing cell membrane with deficiency of the cell wall. The virulence factor for mycoplasma pneumoniae may include P1 adhesion protein. P1 adhesion protein will bind to the epithelial cells which lead to reduction in ciliated clearance, ciliostasis and destruction of the cells. Mycoplasma pneumoniae may cause upper respiratory tract infection such as otitis media, pharyngitis and tracheobronchitis and lower respiratory tract infection. The common mode of transmission is inhalation of the respiratory droplets.Mycoplasma pneumoniae may also present with rashes. The common treatment may include antibiotics such as erythromycin and tetracycline.  Pneumococcal pneumonia Pneumococcal pneumonia is caused by streptococcus pneumoniae. Streptococcus pneumoniae is a gram positive diplococci, sensitive to optochin and bile and alpha hemolytic. The virulence factors of streptococcus pneumoniae may include secretory IgA protease, antiphagocytic polysaccharides capsues, phosphorylcholine and pneumolysin. These virulence factors may promotes cellular invasion and inhibit phagocytic killing. The component of the cell wall such as teichoic acid and peptidoglycan may induce the inflammatory response to the host. The common mode of transmission is via respiratory droplets, organism aspiration from the oropharynx and due to direct contact. Patient with pneumococcal pneumonia may present with sudden onset of fever, shortness of breath, chills, bloody sputum and productive cough. Lobar pneumococcal pneumonia is the commonest form. There are over 80 serotypes of streptococcus pneumoniae based on the polysaccharide capsule. There is a conjugated vaccine against 7 serotypes and polyvalent vaccine against 23 serotypes of streptococcus pneumoniae. Streptococcus pneumoniae may also cause meningitis, otitis media and sinusitis. The treatments may include erythromycin, chloramphenicol and vancomycin.
Neisseria meningitidis infection Neisseria meningitidis is a form of gram negative diplococcus. Respiratory droplets are the common mode of transmission. Gram stain, chocolate agar and blood agar can be useful in identifying Neisseria meningitidis. Latex agglutination test is useful to diagnose neisseria meningitidis in cerebrospinal fluid. Neisseria meningitidis may present with septicemia which may present with ecchymosis and petechiae as well as meningitis. The common complication of neisseria meningitidis infection may include disseminated intravascular coagulation. There are five serogroups of neisseria meningitidis which include A, B, C, Y and W135. The serogroups are based on the polysaccharides capsules. There are vaccine against the serogroups of neisseria meningitidis except serogroup B . Chemoprophylaxis is considered high risk person with close contact with infected person. The common antibiotics such as third generation cephalosporins and penicillin are considered.  |
Kembara's Health SolutionsDiscovering the world of health and medicine. Archives
June 2023
Categories
All
|




 RSS Feed
RSS Feed